Team:SZU-China/Drug Form

Drug Form

In our background research and actual visits, we found that IBD patients' diet was strictly restricted. Conventional drug treatment only brought limited efficacy to patients. Patients often suffer from side effects, high cost, long cycle of treatment, and other physical and mental pain, which leads to low quality of life. As a kind of customized live engineering bacteria adjuvant to prevent recurrence and maintain IBD remission, we hope to pay attention to patients themselves and enhance their medication compliance and invisibility. At the same time, we hope to enhance drug stability while maintaining drug activity to the maximum extent, so as to ease drug storage conditions, reduce the cost of drug manufacturing, transportation and achieve higher economic benefits.
Through the population survey, we found that for long-term drug users, most of them hope that the drugs they take can have strong concealment, small and portable. Therefore, we hope to make an enteric-soluble microcapsule, in which the bacterial powder is embedded, to ensure the recovery activity of the bacterial community after entering the human body and to ensure the therapeutic effect of drugs.
After visiting the microbial pharmaceutical company and discussing with experts, we finally chose the vacuum freeze-drying method as our living bacteria preparation form. Firstly, vacuum-freeze-dried powder has the characteristics of small volume, which can be used to prepare relatively small capsules. Secondly, vacuum freeze-drying powder has excellent stability and recovery activity. For engineering bacteria, the preparation process of freeze-drying technology is relatively stable and mature. The freeze-drying technology can ensure that its plasmids do not lose and continue to express after recovery. Finally, vacuum freeze-drying requires a series of experiments on the strain chassis to select the most appropriate protective agent formulation, so as to reduce or avoid cell damage caused by freeze-drying to a large extent, in order to obtain strains with excellent activity while ensuring a reasonable recovery rate.
Design and Validation
For the strain chassis E.coli Nissle 1917 we selected, we designed and optimized different protective agent formulations by referring to literature research and combining with the actual experimental results, and prepared lyophilized engineering bacterial powder according to the formulations. The prepared bacterial powder was sealed and stored in a 4°C refrigerator. The survival rate of the strain was determined and recorded at the specified time point. At the same time, we tested the enzyme activity of the resuscitated engineered bacteria powder to determine the activity of the engineered bacteria after lyophilization. Due to the particularity of the expressed substance, we decided to select ONLY SOD as the target of enzyme activity measurement.
After our extensive literature research, we found the formulation of a protective agent for our chassis in a paper on the design of a delivery carrier for living bacteria of anti-tumor drugs (E.coli Nissle 1917). In this paper, a single factor test was designed for the lyophilized protectant. The orthogonal test was conducted for the optimization of the protectant formula. The initial lyophilized protectant, namely the first-generation product, was finally determined, whose formula was 3% sucrose concentration, 14.25% skim milk concentration, and 3% L-ascorbate sodium. As figure 1


Fig.1 The first-generation protective agent. A Formulation. B Lyophilized engineered bacterial powder product.
According to our experimental design, we cultured the E.coli Nissle 1917 that had been transformed into the plasmid and the wild-type that had not been transformed into a plasmid and left a sample for counting after the completion of culture. The counting results are shown in Table 1A. Then we centrifuged the bacteria, added the protective agent for pre-freezing, and took it for lyophilization. After lyophilization, we quickly weighed the quality of the bacteria powder, and the results were shown in Table 1B. Then the freeze-dried powder samples were taken for resuscitation count, and the results were shown in Table 1C.
| Bacterial strain | Nissle WT | Nissle-J-BSH | Nissle-J-LL37 | Nissle-J-SODGST |
|---|---|---|---|---|
| Concentration(CFU/ml) | 5.7*10^9 | 2.93*10^9 | 2.21*10^9 | 1.26*10^9 |
| Bacterial strain | Nissle WT | Nissle-J-BSH | Nissle-J-LL37 | Nissle-J-SODGST |
|---|---|---|---|---|
| Mass(g) | 3.2269 | 3.1088 | 3.2997 | 3.1174 |
| Bacterial strain | Nissle WT | Nissle-J-BSH | Nissle-J-LL37 | Nissle-J-SODGST |
|---|---|---|---|---|
| Concentration(CFU/g) | 7.8*10^8 | 5.4*10^8 | 2.41*10^8 | 9.3*10^7 |
Table.1 A Results of engineering bacteria count before lyophilization.
Table.1 B Weighing results of engineering bacteria after lyophilization.
Table.1 C Results of engineering bacteria count after lyophilization.
After that, we stored the powder in a refrigerator at 4°C. Subsequently, we performed resuscitation checks on the freeze-dried powder at an interval of 7 days in the first two weeks and 14 days in the second two weeks, as shown in figure 2. According to this result, we can observe that the recovery rate of lyophilized powder can be maintained at 30%-50% within one month. However, this is only about half of the value in the literature. Refer to the existing living bacteria preparations on the market, such as bifidobacterium triplet enteric-soluble capsules. Each capsule requires an order of bacterial colonies of about 10^6 CFU/g. Our freeze-dried powders have orders of magnitude 1,000 times higher. Therefore, it can be judged that this kind of vacuum freeze-drying protective agent formula has a better protective effect on our engineering bacteria.

Fig.2 Change of recovery rate of lyophilized bacterial powder with time.
However, we are still not satisfied with the recovery rate of lyophilized powder after redissolution. At the same time, we noticed that the group whose recovery rate was measured immediately after lyophilization had a low recovery rate. We contacted Dr. Huang Song, a pharmaceutical preparation expert and doctor of food engineering of Xbiome, and discussed with him. (HUMAN PRACTICE)

Fig.3 Interview with Dr. Huang Song.
At the same time, Dr. Huang believed that if we want to improve the activity and product expression efficiency of lyophilized powder after redissolution, we can consider adding some prebiotics into lyophilized powder or protective agent to enhance the activity of the strain. Prebiotics are a class of indigestible food ingredients, such as fructose-oligosaccharides, that are used as nutrients by the normal intestinal flora to selectively stimulate the growth or activity of one or more bacteria in the colon. Prebiotics can stimulate the growth and activity of saccharides using bacteria such as bifidobacterium and lactic acid bacteria and promote the release of organic acids. These organic acids produce an antibacterial environment that inhibits the growth of intestinal pathogens and is beneficial to host health. Prebiotics are also found naturally in many high-fiber foods, including certain fruits, vegetables and grains. At the same time, many IBD animal model studies have confirmed that prebiotics can inhibit intestinal inflammation, lead to changes in the intestinal flora, reduce the release or expression of inflammatory transmitters. Also, it can reduce bacterial translocation, disease activity index and improve intestinal mucosal damage caused by intestinal inflammation.
Based on the results of the previous generation of experiments, Dr. Huang Song suggested we use two methods to optimize the formulation of lyophilized protectants, which resulted in our second and third-generation products.
The second generation of the product replaces 3% sucrose in the unoptimized protective agent formula with 3% oligosaccharides before the freeze-dried operation, as shown in figure 4A.
The third generation of the product is based on the unoptimized protective agent formula of freeze-dried powder. The exact amount of oligosaccharides as sucrose is directly added into the freeze-dried powder and mixed, as shown in figure 4C.


Fig.4 A Generation II protective agent formulation Fig.4 B Generation II lyophilized engineered bacterial powder.


Fig.4 C Generation III protective agent formulation.
Fig.4 D Generation III lyophilized engineered bacterial powder.
According to the above two formulations, we measured the recovery of lyophilized bacterial powder and the enzyme activity after the recovery in the same way as above. First, we measured the quality of lyophilized bacterial powder of the second generation of products, and the results are shown in table 2. At the same time, according to the recovery of lyophilized powder in different schemes, we carried out the gradient concentration counting. The counting results presented in the second generation were shown in figure 5A. It was found that the recovery rate of each group decreased to varying degrees after the addition of fructose-oligosaccharides, but the overall decline in recovery rate was about one order of magnitude (Unit CFU/g), which had little influence on the actual drug administration. The counting results presented by the third generation product are shown in figure 5B. It can be found that the recovery rate of the other groups increased to varying degrees after the addition of fructose-oligosaccharides except for the LL37 group, and the increase rate of the BSH group even nearly doubled.
| Bacterial strain | Nissle-J-Tes4 | Nissle-J-BSH | Nissle-J-LL37 | Nissle-J-SODGST |
|---|---|---|---|---|
| Mass(g) | 1.82 | 1.83 | 1.74 | 1.79 |
| Bacterial strain | Nissle-J-Tes4Δ | Nissle-J-BSHΔ | Nissle-J-LL37Δ | Nissle-J-SODGSTΔ |
| Mass(g) | 1.32 | 1.31 | 1.29 | 1.35 |
Table.2 The quality of lyophilized powder of the second generation of products (compared with the first generation of lyophilized powder,
the formula quality was halved), where Δ was not added as the first-generation formula control group, and Δ was added as the second-generation formula experimental group.


Fig.5 Recovery rates of different products.
A Generation II. B Generation III.
We further tested the SOD enzyme activity of the engineered bacteria treated by the two methods.
As shown in table 3 and figure 6, the enzyme activity per unit resuscitation volume increased more than twice with the addition of fructose-oligosaccharides regardless of the method used. In terms of the total enzyme activity of the bacteria, the third generation and the second generation are almost the same. However, the amount of bacteria resuscitated in the second generation is nearly ten times that in the third generation, so the enzyme activity per unit resuscitated amount of the second generation is not very good. By comparison, the effect of directly adding fructose-oligosaccharides equal to sucrose into the bacteria powder in the third generation is better. The highest enzyme activity per unit resuscitation was 5.2686x108 CFU/ mL.
Table.3 SOD enzyme activity of resuscitated engineering bacteria of three generations of products


Fig.6 Enzyme activity per recovery of different product.
A Generation II. B Generation III.
Therefore, we can finally determine that the third generation has a higher enzyme activity per unit of recovery volume compared with the second generation on the premise of a slight difference in recovery rate. Therefore, we decided to adopt the third-generation formula. That is, according to the unoptimized protective agent formula of freeze-dried powder, the same amount of oligosaccharides as sucrose was directly added into the mushroom powder and mixed. So far, we have completed the whole process of optimizing the formulation of lyophilized bacterial powder protectants.
The vacuum freeze-drying technology we have mastered brings great convenience to our microcapsule preparation. We only need to mix the bacterial powder with the appropriate capsule material into a solution and then mix it evenly with the core after sterilization. Finally, the mixture of the core material and the capsule material is extruded into fine drops or sprayed into the curing agent solution, slowly stirred and assimilated, and finally collect the microcapsules. What we need to ensure is that our microcapsules are enteric-soluble, as shown in figure 7.

Fig.7 Enteric-soluble microcapsules.
Design
To ensure that the powder does not get broken down or digested elsewhere in the body, such as the stomach, we use hydroxypropyl methylcellulose capsules to bury our powder. Using hydroxypropyl methylcellulose ensures that our capsules can withstand stomach acid and disintegrate in the gut. Therefore, we designed a series of experiments according to The Chinese Pharmacopoeia to verify its enteric solubility and reliability.
According to our clinical investigation, we learned that there was an accumulation of acetic acid and lactic acid in the colon of IBD patients, and the environment was acidic. It was known that the pH of UC patients was lower than 5.7, while the pH of CD patients was also around 5.2, while the pH of the terminal colon of normal people was 7.1-7.5. Some findings also indicate that the colonic pH of UC patients may be related to the severity of the disease [6]. Therefore, we adjusted the pH (pH=6.8, pH=6.6, pH=5.8) of artificial intestinal fluid based on the time limit test of the intestinal disintegrating capsule in The Chinese Pharmacopoeia. The disintegration of enteric-soluble hydroxypropyl methylcellulose capsules was experimentally verified under different pH conditions, as shown in figure 8.

Fig.8 Experiment for disintegration of enteric-soluble capsules.
Validation
In order to conduct targeted drug stability verification for IBD patients with different colon pH at different stages of the disease, we formulated artificial intestinal fluid with three pH gradients according to Chinese Pharmacopoeia. At the same time, we cooperated with Xbiome to conduct standardized and standardized disintegrating time limit examination of enteric-soluble capsules in their Grade C sterile laboratory by using a disintegrating instrument. According to the requirements of The Chinese Pharmacopoeia, the disintegration verification results of enteric-soluble capsules were obtained by naked eye observation, so we filmed the experimental process and results to prove our results.
First, we carried out enteric-soluble capsule embedding of bacterial powder. Due to problems in the experimental environment, we could not use our bacterial powder for the embedding experiment, so we used agar powder to simulate the powder in capsules. We used enteric-soluble hydroxypropyl methylcellulose capsules of size 2, and filled the capsules with a special spoon. The filling volume of each capsule was 100mg, as shown in figure 9.

Fig.9 Enteric-soluble capsule.
After the capsules were filled, we began step 1 of the experiment, which was checked in the hydrochloric acid solution (9:1000) without baffle for 2 hours. At this time, there should not have any crack or disintegration on each capsule shell. As shown in figure 10, the capsules in the three beakers did not disintegrate.




Fig.10 The condition of the capsules after step 1. A All beakers. B Beaker1. C Beaker2. D Beaker3.
We then took out the hanging basket, washed it with a small amount of water, and checked it in phosphate buffer solution 1, 2 and 3 in accordance with the above method, as shown in Figure 24, all capsules should disintegrate within 1 hour. If one cannot completely disintegrate, another 6 should be taken for a retest, which should meet the requirements. In the actual operation, the disintegration time only lasted for 30min. However, all capsules were found to have disintegrated, indicating that enteric-soluble capsules could disintegrate in the intestinal environment of different pH, and the experiment was successful. This experiment showed that the enteric dissolved capsules we selected could disintegrate and take effect in the intestines of IBD patients with different pH, thus confirming the reliability and stability of

Fig.11 Step 2 in progress.

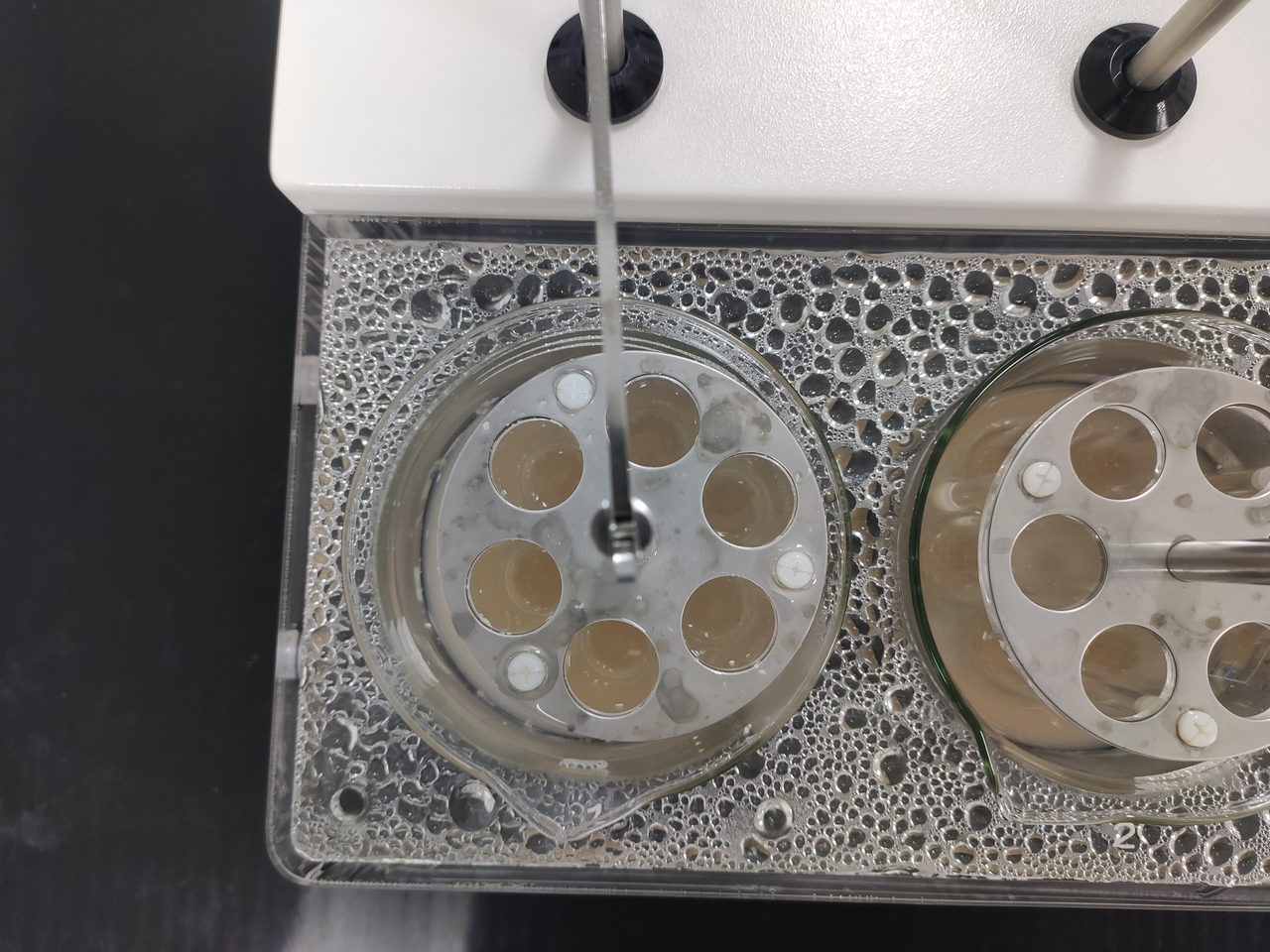

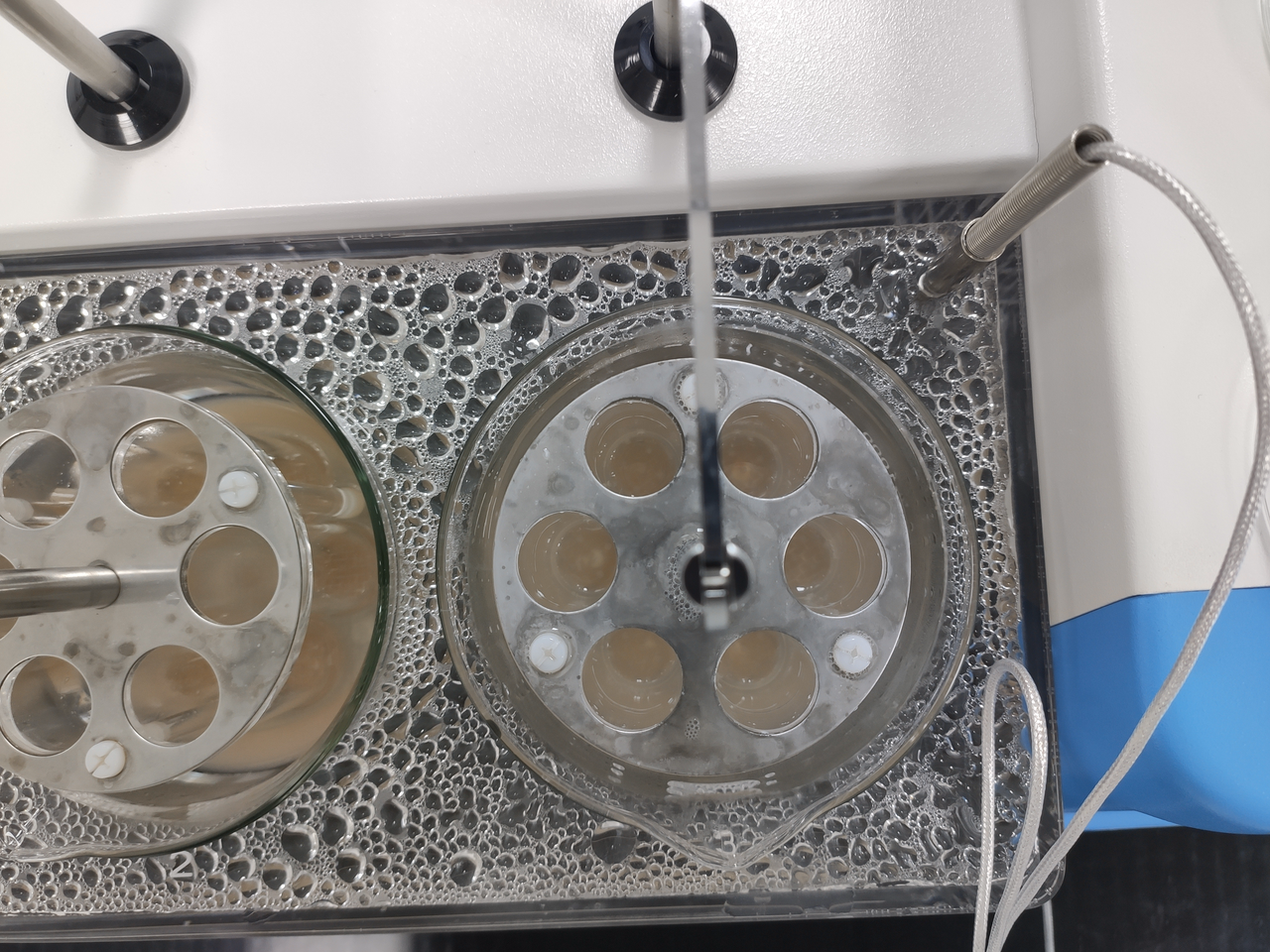
Fig.12 The condition of the capsules after step 2. A All beakers. B Beaker1. C Beaker2. D Beaker3.
The above operation process is in accordance with the guidance of The Chinese Pharmacopoeia[7].

Fig.13 Enteric-soluble lyophilized engineered bacterial powder capsule.
So far, we have completed the design and fabrication of the drug form part of our hardware. To put it simply, in our design, we start from the practical application value of the product, starting from two different entry points of patients and pharmaceutical companies. With the concept of quality and quantity and service to patients, our products are designed and manufactured, and optimized. Our products can be directly used in the production of various preparations and added to food and beverage through different sizes of the design, which can significantly expand the application range of our products. We believe that we have not only completed a vacuum freeze-drying program of E.coli Nissle 1917 engineering bacteria with high maturity, but also made an outstanding contribution to the subsequent application of microcapsule technology in E.coli Nissle 1917 engineering bacteria.
But we hope we can do better in the future. More precise and targeted experiments and product validation are waiting for us. We believe that our work is only a tiny step, and we will have the courage to challenge the next mountain in order to create better products with the spirit of artisans.
[1] Ren Yan, Chen Ming et al. Influence of protectants on the survival of Lactic acid bacteria during the vacuum freeze-drying process[J].China Dairy Industry, 2013,41(09):41-45.
[2] Can W. Optimization of fermentation process of Anti-tumor engineering NISSLE 1917 and preparation of bacterial powder[D]. Hunan Norman University, 2017.
[3] Oliver, J. D. (2005). The viable but nonculturable state in bacteria. Journal of microbiology, 43(spc1), 93-100.
[4] Jie Z, Weiming Z, Ning L. Probiotics, Prebiotics, Synbiotics and inflammatory bowel disease[J]. Parenteral & Enteral Nutrition, 2014, 21(04):251-153+256.
[5] Nugent SG, Kumar D, Rampton DS, Evans DF. Intestinal luminal pH in inflammatory bowel disease: possible determinants and implications for therapy with aminosalicylates and other drugs[J]. Gut. 2001;48(4):571-577. doi:10.1136/gut.48.4.571
[6] 陈宇洲,王东凯.炎症性肠病的结肠生理特征和结肠定位给药[J].Chinese Pharmaceutical Journal,2006(02):86-90.
[7] 国家药典委员会.中国药典[M].北京:中国医药科技出版社,2020:129-130.
[8] National Health Service (NHS). Inflammatory bowel disease[EB/OL]. 2020[2021.9.30].
[9] Group I B D, Gastroenterology C S O, Association C M. Chinese consensus on diagnosis and treatment of inflammatory bowel disease(Beijing, 2018)[J]. Chinese Journal of Practical Internal Medicine, 2018.9, 38(9):796-813.

